This study aimed to find out how well a single dose of creatine (0.2 g/kg) mitigates cognitive decline under sleep deprivation. The results showed that creatine supplementation had a positive effect on reducing sleep-deprivation-induced cognitive deterioration in logic and numerical tasks, verbal processing speed, and the Psychomotor Vigilance Task (PVT). Female participants notably showed greater benefits than male participants.
1. Introduction: Creatine's Diverse Benefits and Research Background 💡
Creatine was originally used as a supplement to enhance athletic performance, but recent research has demonstrated its therapeutic effects and clinical relevance in areas including traumatic brain injury, neurodegenerative disease, tumor suppression, and depression. It has been shown to positively influence brain function and cognitive performance, to help with neuro-cognitive and metabolic changes in menopausal women, and to be beneficial under conditions of sleep deprivation, fatigue, and cognitive impairment. Creatine modulates neural excitability and neurotransmission, possesses neuroprotective properties, and exerts neuroprotective effects through antioxidant activity.
However, a challenge remained: in healthy individuals, oral creatine does not greatly raise brain creatine levels, and the low central nervous system uptake rate means that at least one week of oral creatine intake is typically needed to improve cognitive performance.
Earlier research showed that a high single dose of creatine (0.35 g/kg) induced metabolic changes and attenuated cognitive decline during sleep deprivation. Cellular stress caused by sleep loss and high extracellular creatine availability appeared to be the key factors driving increased creatine uptake. This study set out to determine whether a lower dose (0.2 g/kg) can produce the same effect, focusing exclusively on cognitive performance outcomes — important information for minimizing side effects and improving safety.
2. Materials and Methods: Participants and Experimental Procedure 🧪
2.1. Participants 👨👩👧👦
Twenty-nine healthy participants took part in the study (17 female, 9 vegetarian, mean age 27 years). Participants had no history of sleep disorders, psychiatric or neurological conditions, or alcohol or substance abuse, and were non-smokers taking no medications. They were asked to stop caffeine and alcohol consumption 48 hours before the experiment and were instructed to sleep at least 7 hours per night, go to bed before midnight, and wake at 7 a.m. for the two weeks prior to the experiment. All participants provided informed consent in accordance with the Declaration of Helsinki.
2.2. Experimental Procedure 🗓️
The study used a double-blind, randomized, crossover design. Participants completed two measurement nights separated by 7 days; on one night they received 0.2 g/kg creatine monohydrate, and on the other they received the same dose of placebo. The research team continuously supervised participants to ensure they remained sleep-deprived, and cognitively stressful activities were prohibited. Water and non-meat snacks were permitted.
The experimental timeline was as follows:
- 6:33 PM (baseline): First cognitive assessment begins
- 9:00 PM: Creatine or placebo ingested
- 11:33 PM, 2:29 AM, 4:29 AM: Additional cognitive assessments (each taking approximately 22 minutes 48 seconds)
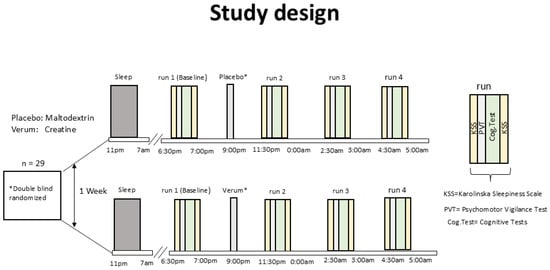
 Figure 1. Study design: double-blind, randomized, crossover design in which participants ingested creatine or placebo at 9 PM. Cognitive assessments were conducted four times: at baseline (6:30 PM), 11:30 PM, 2:30 AM, and 4:30 AM.
Figure 1. Study design: double-blind, randomized, crossover design in which participants ingested creatine or placebo at 9 PM. Cognitive assessments were conducted four times: at baseline (6:30 PM), 11:30 PM, 2:30 AM, and 4:30 AM.
2.2.1. Cognitive Scores and Tasks 🧠📝
Before each assessment, participants completed the Karolinska Sleepiness Scale (KSS) and the Fatigue Scale (FAT). The cognitive tasks were structured as follows:
- Psychomotor Vigilance Task (PVT): An 8-minute task in which participants pressed a mouse button as quickly as possible whenever a number appeared on the screen, measuring reaction time.
- Memory tasks:
- Word Memory Test (WMT): Participants memorized pairs of German nouns — 22 pairs were presented at 5 seconds each — and were then tested on recall.
- Forward Digit Span (SPAN): Twelve randomly generated single-digit numbers were presented at 5 seconds each, and participants recalled them in the original order.
- Spatial N-back (2-back): Squares appeared sequentially in a 3×3 grid, and participants judged whether the current square matched the one from two steps back.
- Multiple-choice cognitive test: Multiple-choice questions covering verbal (21 items), logical (17 items), and numerical (9 items) ability. Verbal sub-categories included analogies, word ordering, and finding words with a common general term; logic tasks included completing figure patterns and mental rotation; numerical tasks included completing number sequences and addition.
2.3. Statistics and Analysis 📊
Data were analyzed using linear mixed models (LMM), and a difference-in-differences (DiD) approach was used to compare within-person changes between creatine and placebo under sleep deprivation. Bonferroni correction was applied to control for multiple comparison errors.
3. Results: Creatine's Cognitive Protection Effects 🚀
All participants successfully completed the study, and no gastrointestinal problems or other adverse effects were reported following creatine supplementation. Sleep deprivation significantly increased participants' fatigue levels.
3.1. Linear Mixed Model (LMM) Results 📈
In the placebo condition, sleep deprivation produced significant changes (deterioration) from baseline in logic, PVT (mean reaction time, median reaction time, reaction time variability), WMT, SPAN, KSS, and FAT scores as the night progressed. In the creatine condition, an interaction effect was observed only for the logic task and PVT (mean reaction time variability). Notably, creatine significantly attenuated the slope of cognitive decline in the logic task compared to placebo: the rate of decline was 0.126 per hour in the placebo group, but only 0.015 in the creatine group — a dramatic reduction.
3.2. Difference-in-Differences (DiD) Analysis Results 📉
3.2.1. Cognitive Response to Sleep Deprivation 😴
KSS and FAT scores in the placebo group increased continuously from baseline, showing deepening fatigue. At the final time point (4 AM), KSS scores had risen by 173% and FAT scores by 115%. Significant performance decrements were also observed in memory tasks (WMT, SPAN), the logic task, and PVT reaction times. A significant positive correlation emerged between increasing fatigue and worsening reaction-time performance.
3.2.2. Cognitive Response to Sleep Deprivation After Creatine 💪
After creatine ingestion, KSS and FAT scores still increased from baseline, reflecting higher fatigue levels, but improvement effects appeared in some cognitive tasks.
- Numerical tasks showed a 6.9% performance improvement.
- Verbal processing speed improved by 8.0%, and logic task processing speed by 10.1%.
- At 4 AM in particular, logic task processing speed was 16.3% higher.
However, most single-timepoint changes did not remain significant after Bonferroni correction.
3.2.3. Creatine vs. Placebo Cognitive Response Comparison ⚔️
Compared with placebo, creatine produced the following cognitive performance improvements:
- Logic task: 6.1% improvement 📈
- Numerical task: 6.2% improvement 📈
- Verbal processing speed: 12.3% improvement 📈
- PVT reaction time variability (RTD): 9.2% improvement 📈 (indicating more consistent reaction times)
 Figure 3. Percentage change from baseline (6 PM) in cognitive performance for placebo (grey), creatine (red), and creatine vs. placebo (combined across three time points) during sleep deprivation. Positive values indicate improved performance; negative values indicate decline.
Figure 3. Percentage change from baseline (6 PM) in cognitive performance for placebo (grey), creatine (red), and creatine vs. placebo (combined across three time points) during sleep deprivation. Positive values indicate improved performance; negative values indicate decline.
Female participants showed significant improvements of 12.3% in the logic task, 18.2% in verbal processing speed, 10.3% in logic processing speed, and 3.2–9.6% in PVT (RTD, mean reaction time, median reaction time, speed). Vegetarians showed improvement in the N-back task, verbal task processing speed, and PVT (slowest 10% reaction times), while non-vegetarians showed improvement in logic and numerical tasks.
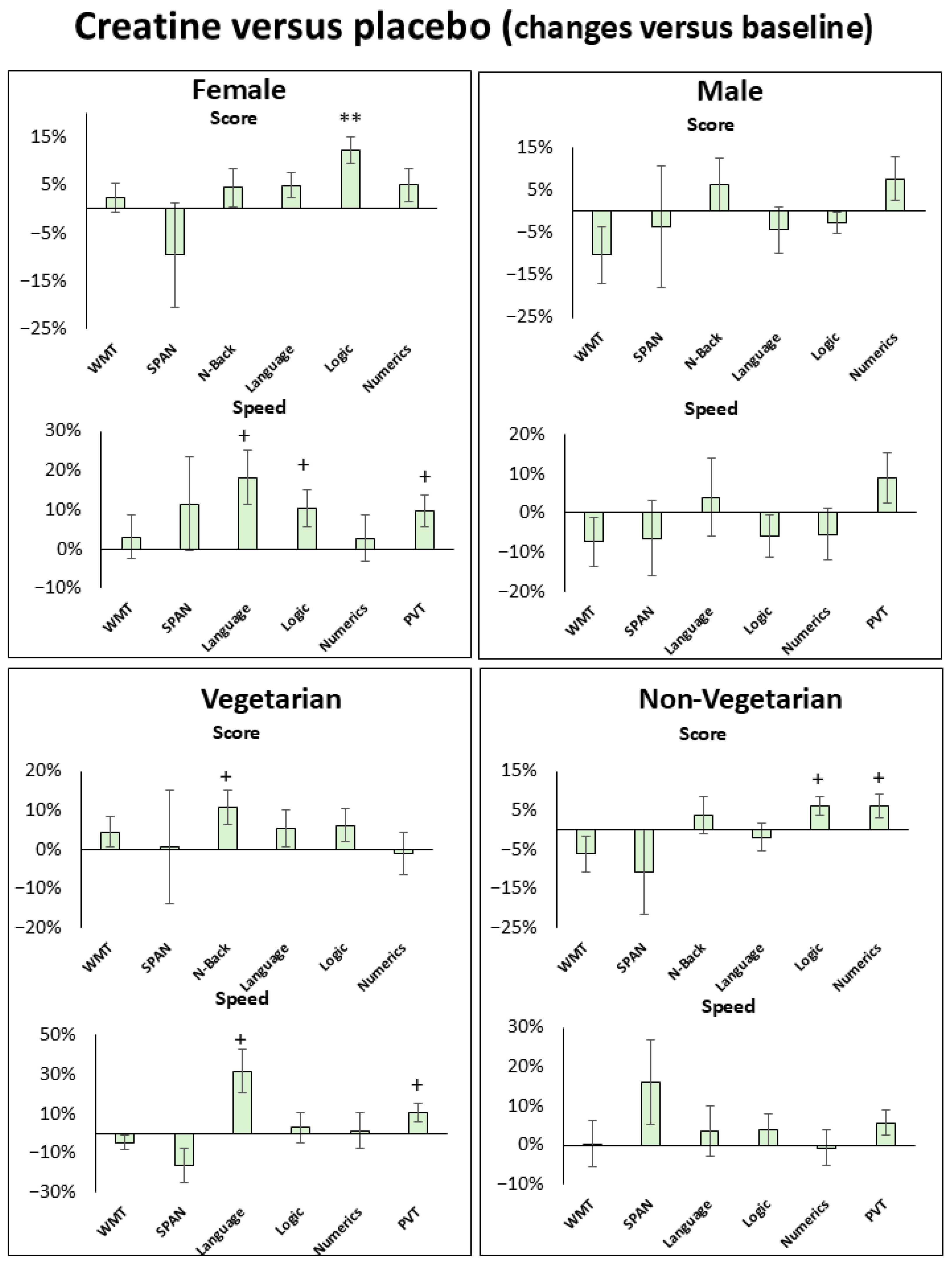 Figure 6. Percentage change from baseline (6 PM) in cognitive performance under sleep deprivation for creatine vs. placebo, shown separately for female, male, vegetarian, and non-vegetarian groups. Positive values indicate improved performance; negative values indicate decline.
Figure 6. Percentage change from baseline (6 PM) in cognitive performance under sleep deprivation for creatine vs. placebo, shown separately for female, male, vegetarian, and non-vegetarian groups. Positive values indicate improved performance; negative values indicate decline.
4. Discussion: Creatine Dose, Sex, and Personalized Strategies 🧐
This study demonstrated that a single oral dose of 0.2 g/kg creatine can attenuate sleep-deprivation-induced cognitive decline. This corroborates the effects of higher-dose creatine established in previous research and suggests that cellular stress during sleep deprivation, combined with adequate extracellular creatine availability, is important for cognitive improvement.
However, the lower dose used here produced weaker effects than those seen in prior high-dose studies. Whereas the earlier research found the strongest effects in short-term memory tasks and processing speed, this study saw more pronounced effects in working memory domains such as PVT and logic tasks. This implies that creatine's effects may vary by dose — analogous to how creatine maintains ATP levels and limits lactate accumulation to sustain peak performance during intense physical exercise.
Regarding the dose-response relationship: blood creatine concentrations rise linearly with ingested dose and peak approximately 3 hours after ingestion. Because neuronal uptake is far lower than muscular uptake, the impact of a lower dose on cognitive performance may be limited. This study confirmed that 0.2 g/kg creatine is a safe dose, and up to a 12% improvement in cognitive performance was observed.
The most striking finding was the sex difference. Female participants responded more sensitively to creatine than male participants, showing greater attenuation of cognitive decline — particularly in logic tasks, verbal and logic processing speed, and PVT. This suggests that women may derive greater benefit from the bioenergetic support that creatine provides during acute sleep deprivation.
"Women appeared to be less affected by cognitive decline than men — particularly in processing speed and reaction time (PVT)."
This resilience of women to sleep deprivation and fatigue has been observed in other research and may involve neural activity in specific brain regions (right prefrontal cortex). Additionally, women's baseline brain creatine levels are lower than men's, and creatine levels fluctuate with estrogen, which may account for this heightened sensitivity. A further hypothesis is that the SLC6A8 transporter gene — critical for creatine uptake — is located on the X chromosome, so genetic variation in women may result in different transporter levels.
Significant improvements were also found in the vegetarian and non-vegetarian subgroups, though not as pronounced as the sex differences. Like women, vegetarians showed improvements in processing speed, supporting the hypothesis that both groups have lower baseline creatine levels and therefore stand to gain more from supplementation.
The study has several limitations: the sample size was relatively small, brain creatine levels were not measured directly, and the study was restricted to young adults, making generalization to older populations difficult. Nevertheless, these findings provide an important foundation for developing personalized supplementation strategies in future research. Groups with characteristically lower creatine stores — women, vegetarians, and older adults — are expected to benefit most from creatine supplementation during sleep deprivation. The findings also suggest that athletes and coaches need dose-tiered strategies to mitigate sleep-deprivation-induced cognitive decline: a moderate dose offers gradual improvement, but tasks requiring high processing speed may call for a higher dose.
5. Conclusion: Cognitive Benefits of 0.2 g/kg Creatine Under Sleep Deprivation and Future Directions 🌟
This study showed that a single 0.2 g/kg dose of creatine modestly attenuates cognitive decline under sleep deprivation. Although the effect size was not large, up to a 12% improvement in cognitive performance was observed. These improvements were most pronounced in logic, numerical ability, verbal task processing speed, and the Psychomotor Vigilance Task (PVT).
In particular, women gained greater benefits than men in logic tasks, PVT, and verbal and logic processing speed. The results suggest that creatine uptake by brain cells and the resulting cognitive improvements may vary by dose. Since 0.2 g/kg creatine has been confirmed as a safe dose, future research should explore adding complementary compounds or modifying creatine formulations to increase cellular uptake and amplify effects. Furthermore, these findings can serve as a foundation for additional studies determining personalized creatine dosing for diverse populations.