This is a prospective cohort study analyzing the association between muscular strength and mortality in 5,472 ambulatory women aged 63 to 99. The results show that higher muscular strength, measured by grip strength and chair-stand time, is significantly associated with lower all-cause mortality risk. Notably, these associations persisted after adjusting for physical activity, sedentary time, walking speed, and inflammation levels — and even appeared in women who did not meet physical activity guidelines.
1. Background and Objectives
The 2018 U.S. Physical Activity Guidelines and the 2024 AHA Scientific Statement recommend at least two weekly sessions of muscle-strengthening activity. While prior studies demonstrated an inverse relationship between muscular strength and mortality, most relied on self-reported physical activity data and failed to adequately control for cardiorespiratory fitness.
This study's primary objective was to determine the association between muscular strength and all-cause mortality in ambulatory women aged 63 to 99, while controlling for accelerometer-measured physical activity, sedentary time, walking speed (a proxy for cardiorespiratory fitness), and systemic inflammation.
2. Methodology
2.1. Study Design and Participants
A prospective cohort study from the OPACH (Objective Physical Activity and Cardiovascular Health) study, conducted from March 2012 to April 2014, with follow-up through February 19, 2023. A total of 5,472 ambulatory women aged 63-99 completed physical performance testing and wore accelerometers for 7 days.
2.2. Strength Measurements
Two standard measures were used:
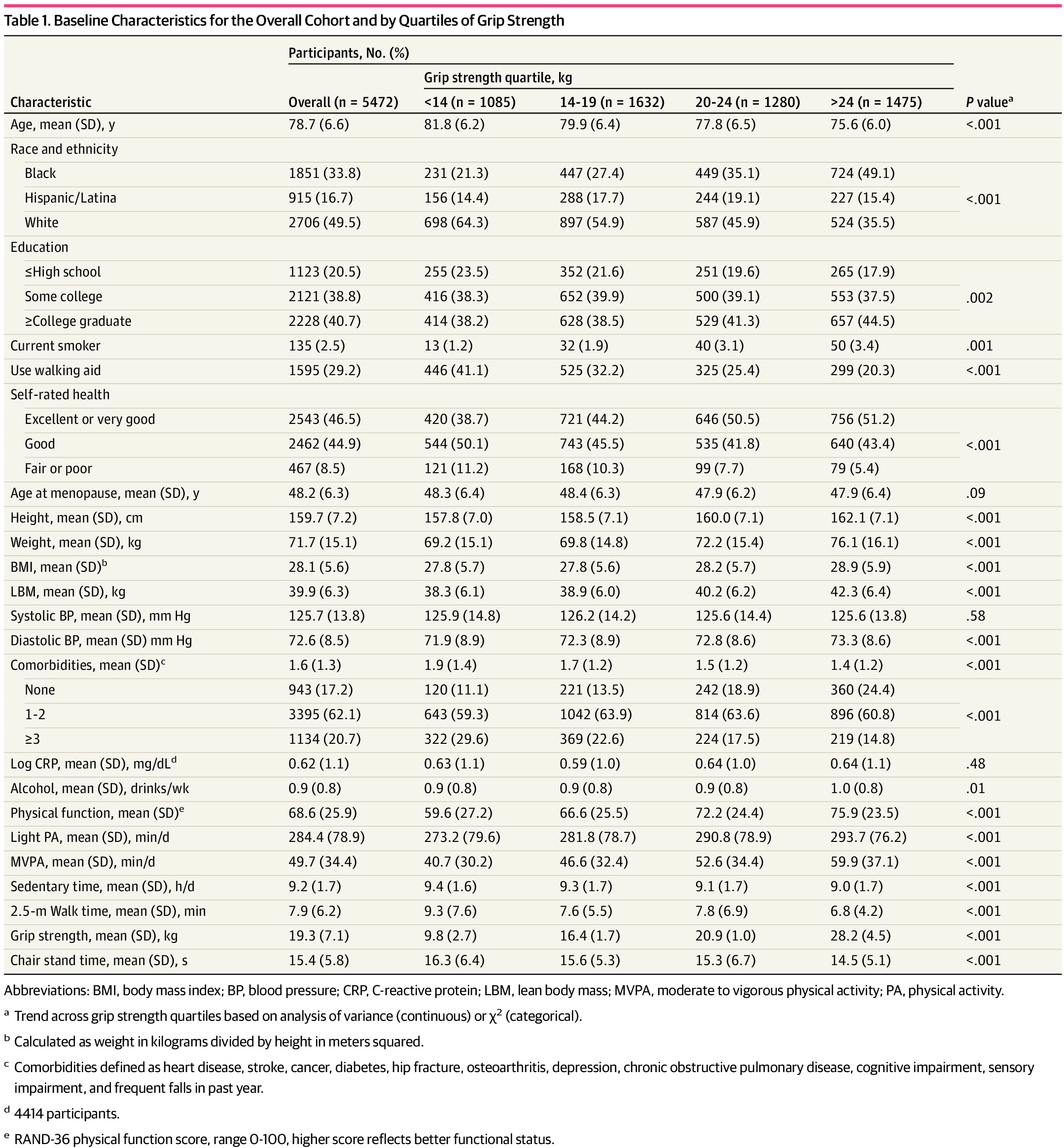
- Grip strength: Measured using a dynamometer on the dominant hand. The highest of two attempts was recorded and categorized into quartiles (Q1: <14kg, Q2: 14-19kg, Q3: 20-24kg, Q4: >24kg).
- Chair-stand time: Time to complete 5 consecutive sit-to-stand repetitions with arms crossed, also categorized into quartiles (Q1: >16.7s slowest, Q4: ≤11.1s fastest).
2.3. Mortality and Covariates
All-cause mortality was tracked through annual health updates and death record searches. Confounders included age, race/ethnicity, education, weight, blood pressure, comorbidity count, alcohol use, menopause age, walking aid use, smoking, and self-rated health. Accelerometer-measured physical activity (light and MVPA), sedentary time, 2.5m walk time, and C-reactive protein (CRP) levels were also analyzed.
3. Results
3.1. Participant Characteristics
Mean age was 78.7 years. The cohort comprised 33.8% Black, 16.7% Hispanic/Latina, and 49.5% White women. Approximately 79.4% had college education or higher, 29% used walking aids, and mean grip strength was 19.3kg with mean chair-stand time of 15.4 seconds.
3.2. Strength-Mortality Association
Over a mean follow-up of 8.3 years, 1,964 (35.8%) women died.
- Grip strength: A clear inverse dose-response trend — the highest quartile had 67% lower mortality risk compared to the lowest (HR: 0.67, 95% CI: 0.58-0.78, p < 0.001).
- Chair-stand time: The fastest quartile had 63% lower mortality risk versus the slowest (HR: 0.63, 95% CI: 0.54-0.73, p < 0.001).
These associations persisted after simultaneously adjusting for accelerometer-measured sedentary time, MVPA, walking speed, and CRP. Women who did not meet physical activity guidelines (MVPA <150 min/week) still showed lower mortality with higher grip strength — suggesting strength training may be especially valuable for those unable to perform aerobic exercise.
"Muscular strength was associated with lower mortality even among women who did not meet physical activity guideline recommendations."
4. Discussion and Implications
This study provides robust evidence that muscular strength independently predicts lower all-cause mortality in older women, above and beyond physical activity, cardiorespiratory fitness, and inflammation.
- Grip strength (upper body) and chair-stand time (lower body) were weakly correlated, indicating they capture different dimensions of strength.
- Objective accelerometer measurements overcame limitations of self-reported data in prior studies.
- The finding that strength matters even for guideline-noncompliant women suggests strength maintenance is a feasible longevity strategy for those with limited mobility.
4.1. Limitations
- Only two strength measures used (no isokinetic or 1-RM testing).
- Lean body mass was estimated, not directly measured via imaging.
- Nutritional status was not systematically collected.
- Results are from postmenopausal women in the WHI and may not generalize to men or younger women.
Conclusion
Higher muscular strength is clearly associated with significantly lower all-cause mortality in ambulatory women aged 63 to 99. This relationship holds independently of physical activity, walking speed, and inflammation, and is present even in women not meeting activity guidelines. Routine strength assessment in clinical settings and encouraging strength maintenance could play a critical role in healthy aging and longevity for older women.