This study explores the complex relationship between heart rate variability (HRV), neurological health, and cognitive function. HRV is a metric that measures the subtle time variations between heartbeats, reflecting autonomic nervous system activity and closely linked to various cognitive functions including executive function, decision-making, and emotion regulation. Importantly, when interpreting HRV changes due to aging or cardiovascular disease, it is essential to consider irregular sinus rhythms (heart rate fragmentation, HRF), which can lead to overestimation of autonomic nervous activity. This review illuminates the abnormal HRV changes observed across several neurological conditions including dementia, mild traumatic brain injury, migraine, COVID-19, stroke, epilepsy, and psychological states such as anxiety, stress, and schizophrenia.
1. Heart-Brain Interaction and Introduction to Heart Rate Variability (HRV)
The heart and brain are intimately connected, influencing each other through both electrical and hemodynamic pathways. For example, the vagus nerve is primarily distributed to the sinoatrial and atrioventricular nodes of the heart, releasing acetylcholine to slow heart rate, while sympathetic nerves release norepinephrine and epinephrine to accelerate heart rate. The speed at which heart rate is modulated depends on how quickly each branch of the autonomic nervous system processes signals -- vagal acetylcholine acts rapidly, greatly influencing beat-to-beat changes, while sympathetic norepinephrine acts more slowly, affecting cardiac rhythm across multiple beats.
Signals traveling from the heart to the brain are also important. Over 80% of vagal nerve fibers are afferent, transmitting information to various brain regions including the brainstem, hypothalamus, thalamus, amygdala, and cerebral cortex.
FIGURE 1.
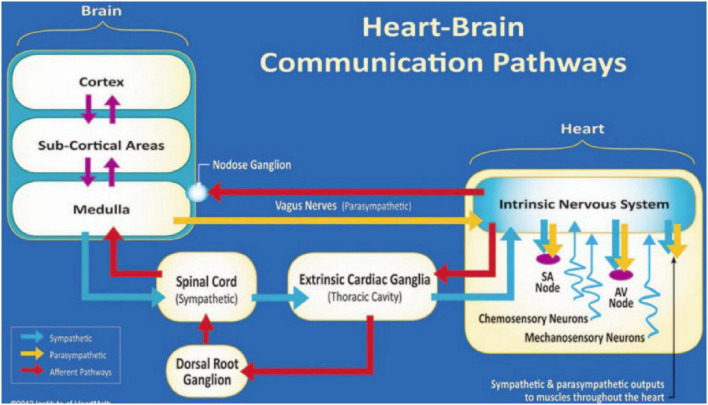 The neural communication pathways between heart and brain are central to HRV generation. The intrinsic cardiac nervous system within the heart integrates information from the extrinsic nervous system and intracardiac sensory neurons, while the vagus nerve (parasympathetic) is composed primarily of afferent fibers flowing to the brain, connecting to the medulla.
The neural communication pathways between heart and brain are central to HRV generation. The intrinsic cardiac nervous system within the heart integrates information from the extrinsic nervous system and intracardiac sensory neurons, while the vagus nerve (parasympathetic) is composed primarily of afferent fibers flowing to the brain, connecting to the medulla.
Beyond electrical connections, hemodynamic connections through blood circulation are also critically important. The heart pumps blood to supply oxygen and nutrients to the brain, while oxygen-depleted blood returns from the brain to the heart for re-oxygenation. When cardiac function is impaired, such as in heart failure, cerebral blood flow decreases, affecting cognitive function and increasing dementia risk. Reduced cardiac output from arrhythmias like atrial fibrillation can also reduce cerebral blood flow, leading to cognitive impairment. Additionally, cardiac thrombi or atherosclerotic lesions can obstruct cerebral blood flow or cause stroke, and hypertension can lead to lacunar infarcts in the brain.
This bidirectional connection between heart and brain significantly affects our physiological, psychological, and cognitive health, playing an important role in physical, mental, and social well-being. For example, natural disaster stress such as earthquakes and pandemics is associated with increased cardiac death and myocardial infarction, and even non-natural factors like sports events can increase cardiac death risk in emotionally engaged fans. Research has also shown that higher Framingham cardiovascular risk scores are associated with increased risk of cerebral infarction, cerebral atherosclerosis, and Alzheimer's disease.
1.1. Heart Rate Variability (HRV)
Heart rate variability (HRV) measures the variation in time intervals between heartbeats (R-R intervals), known as an indicator reflecting the dynamic interplay between sympathetic and parasympathetic nervous activity. It is typically measured by analyzing 1-minute or 5-minute electrocardiogram (ECG) recordings in a resting state. Various software tools such as Kubios and Biopac are used for this analysis.
In HRV analysis, ectopic beats are typically removed to consider only sinus beats that reflect the brain's autonomic neural circuit signals. However, recent research suggests that irregular sinus arrhythmias can affect HRV independently of autonomic regulation, potentially confounding the interpretation of autonomic regulation in traditional HRV analysis. Therefore, these irregular rhythms should be excluded before accurately interpreting autonomic nervous activity.
1.1.1. Traditional HRV Analysis in Time and Frequency Domains
HRV is primarily analyzed using linear methods. In the time domain, measurements include R-R intervals (RR), heart rate (HR), standard deviation of normal-to-normal (NN) intervals (SDNN), root mean square of successive R-R interval differences (RMSSD), and the percentage of successive NN interval changes exceeding 50ms (pNN50).
In the frequency domain, analysis includes high frequency (HF), low frequency (LF), very low frequency (VLF), and ultra-low frequency (ULF). Nonlinear HRV analysis methods also exist but are not the primary focus of this review.
- RMSSD and HF primarily reflect the vagal (parasympathetic) influence on the heart. Higher HF, RMSSD, and pNN50 values indicate more active vagal function, while lower values suggest diminished vagal activity.
- The LF/HF ratio was previously used as an indicator of sympatho-vagal balance, but recent research argues it is not an accurate marker, as LF reflects complex factors beyond sympathetic and parasympathetic activity and is independently influenced by respiration and heart rate. Therefore, this review no longer considers the sympatho-vagal balance interpretation of the LF/HF ratio.
- SDNN represents overall heart rate variability and is more influenced by sympathetic nervous activity than other HRV measures.
- VLF and ULF are primarily analyzed from 24-hour ECGs and are known to be related to circadian rhythms, body temperature, metabolism, and sleep cycles, though research on these remains limited.
This review uses the term "vagal functioning" because additional components of HRV have been reported over the past several decades. HRV also reflects respiratory activity (respiratory sinus arrhythmia, RSA) and blood pressure fluctuations (Mayer waves, approximately 0.1Hz).
TABLE 1.
Traditional HRV time-domain and frequency-domain measurements and heart rate fragmentation measurements.
| Parameter | Unit | Description |
|---|---|---|
| SDNN | ms | Standard deviation of NN intervals |
| pNN50 | % | Percentage of successive RR interval differences exceeding 50ms |
| RMSSD | ms | Root mean square of successive RR interval differences |
| ULF power | ms2 | Absolute power in the ultra-low frequency band (=0.003 Hz) |
| VLF power | ms2 | Absolute power in the very low frequency band (0.0033-0.04 Hz) |
| LF power | ms2 | Absolute power in the low frequency band (0.04-0.15 Hz) |
| LF power | nu | Relative power in the low frequency band in normalized units |
| HF power | ms2 | Absolute power in the high frequency band (0.15-0.4 Hz) |
| HF power | nu | Relative power in the high frequency band in normalized units |
| LF/HF | % | Ratio of LF to HF power |
| PIP | % | Percentage of inflection points in RR intervals |
NN intervals: inter-beat intervals with artifacts removed; RR intervals: all successive heartbeat intervals. ms: milliseconds; ms2: squared milliseconds; nu: normalized units; PIP: percentage of inflection points.
1.1.2. Heart Rate Fragmentation (HRF)
Heart rate fragmentation (HRF) has become an important consideration as complex factors contribute to inter-beat variation, raising concerns that traditional HRV analysis may over-interpret sympatho-vagal balance. In particular, non-respiratory sinus arrhythmias and irregular sinus rhythms affect HRV independently of autonomic regulation, potentially confounding the prognostic role of traditional HRV analysis.
The Costa research team introduced heart rate fragmentation (HRF) analysis (e.g., percentage of inflection points, PIP) to distinguish between irregular rhythms and autonomic regulation. HRF increases with aging and has been shown to provide additional or independent information beyond traditional HRV changes in cardiovascular conditions such as coronary artery disease or cardiovascular disease events. In 2021, the Costa team reported that increased HRF during sleep reflects and predicts decline in overall cognitive ability (CASI) and processing speed (DSC).
This review focuses primarily on RR, HR, RMSSD, SDNN, HF, and LF, but clarifying the roles of HRF and autonomic contributions to HRV in future research will be important.
1.1.3. HRV, Age, Sex, and Heart Rate
HRV measurements are influenced by age and sex. A study of 1,743 participants between ages 40 and 100 found that SDNN decreases with age, while RMSSD decreases from age 40 to 60 and then increases after ages 60-70. Women had lower SDNN but higher RMSSD than men, and diabetic patients of both sexes had lower RMSSD and SDNN.
Another study found that women had higher heart rate and HF (vagal activity) than men, but this difference gradually disappeared with age. Notably, the increase in RMSSD after ages 60-70 may reflect not only vagal function but also irregular rhythms or increased heart rate fragmentation, requiring caution when interpreting such changes in HRV studies involving elderly participants. Therefore, HRV research that accounts for sex and age differences will help improve the reproducibility and reliability of HRV results.
Heart rate (HR) itself can also affect HRV. A study of 36 young healthy volunteers found that HRV depends more on heart rate than respiratory rate, and removing heart rate influence improves HRV repeatability. However, considering that heart rate itself may be a risk factor for cognitive decline, the predictive value of HRV may be either independent of or dependent on heart rate. Thus, heart rate correction is not always used in HRV analysis.
1.2. HRV and the Brain
Interest in the association between HRV and cognitive function has been growing. This report aims to summarize knowledge about the connection between HRV and cognitive function, their interactions in physiological states and neurological conditions, underlying mechanisms, and potential ways to improve overall health through these connections.
FIGURE 2.
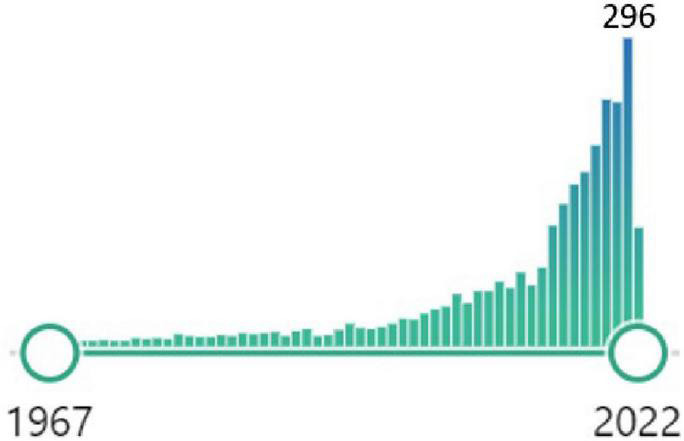 The number of publications on HRV and cognitive function has been increasing in recent years.
The number of publications on HRV and cognitive function has been increasing in recent years.
2. Research Methods
This review examined literature on the association between HRV and cognitive function from PubMed and Google Scholar databases. Search keywords included "heart rate variability," "cognition," "dementia," "Alzheimer's disease," "traumatic brain injury," "migraine," "COVID-19," "stroke," "epilepsy," "psychological states," and "inhibitory control." Additionally, "irregular rhythm" and "heart rate fragmentation" were included as search keywords. Related studies cited in review papers were also examined to compile the final reference list.
Because this review examines heart-brain connections specifically from the perspective of HRV and cognitive function, it may not include all relevant research in this field.
3. HRV Changes and Neurological Conditions
3.1. Physiological Conditions
Heart rate variability (HRV) directly and indirectly influences decision-making related to overall health in daily life. High HRV (high HF or RMSSD measurements) is associated with enhanced executive function, better dietary decisions, ability to control social media use, and negative avoidance ability.
3.1.1. Executive Function
HRV measurements (LF, HF, LF/HF, RMSSD, SDNN) can serve as potential early indicators of cognitive decline. In a study of 79 young healthy participants, high resting HF was associated with higher executive function. Interestingly, low resting heart rate was correlated with higher executive function when controlling for lower-level processes such as processing speed.
Another study of 53 young male sailors found that higher resting RMSSD (higher vagal function) was associated with better working memory and attention (including faster and more accurate responses).
Inhibitory control is measured through responses such as startle reactions to auditory stimuli. In one study, 92 college students had their resting HRV measured while performing working memory tasks and picture viewing tasks. Participants with low resting HF showed greater startle responses under high working memory load. This suggests that when the prefrontal cortex is overloaded by high working memory demands, insufficient top-down resources are available.
Additionally, a study of 50 young healthy participants reported a positive association between resting HRV and inhibitory control. Higher resting RMSSD predicted better inhibitory control even after adjusting for confounding variables such as sex, BMI, and impulsivity. A path modeling study of 8,114 Brazilian civil servants found that decreased HF was associated with executive dysfunction due to insulin resistance and subclinical atherosclerosis.
3.1.2. Decision-Making
A study of 51 young male participants investigated the relationship between resting HRV and dietary decision-making (choosing between healthy nutrients and tempting treats). Those with higher HRV better resisted the temptation of appetizing food, and functional MRI showed higher ventromedial prefrontal cortex activity, supporting HRV as a strong biomarker of dietary self-control.
Another decision-making example relates to restraining social media overuse. In a study of 112 participants aged 17 to 53, those with higher impulsivity and lower executive function scores tended to suffer from social media overuse. Interestingly, higher HRV was associated with reduced impulsivity. Thus, higher HRV can help resist social media overuse both directly and indirectly through better executive function and lower impulsivity.
3.1.3. Emotion Regulation
Decision-making is influenced by emotion regulation. In a study of 63 young participants (mean age 19) and 62 older participants (mean age 72), resting HRV and eye tracking were measured while showing facial images expressing various emotions. Young participants showed no preference for happy or angry faces regardless of HRV level, but older participants with higher HRV showed a tendency to avoid angry faces more. This suggests greater ability to minimize negative affect and a stronger positivity effect that benefits emotion regulation and health.
Another study using fMRI and HRV methods with 21 older adults and 20 young adults showed that higher resting HRV (RMSSD) was associated with stronger amygdala-medial prefrontal cortex (mPFC) connectivity across age groups. However, amygdala-ventrolateral prefrontal cortex connectivity was stronger only in the young group. This study indicates that higher HRV is associated with better emotion regulation across age groups, with some regional associations changing during aging.
A study of 388 healthy participants across three different age groups suggested that higher RMSSD was associated with higher functional connectivity in bilateral ventromedial prefrontal cortex in the young adult group and higher functional connectivity in bilateral posterior cingulate cortex across all ages. This supports the role of prefrontal cortex functional plasticity during aging.
Therefore, vagal function associated with higher HRV provides healthy individuals with better executive function, decision-making ability, and emotion regulation, benefiting health and well-being. Additionally, cognitive function (prefrontal cortex connectivity) can change with aging, but emotion regulation is robust to aging.
3.2. Pathological Conditions: Dementia, Traumatic Brain Injury (TBI), Migraine, COVID-19, Stroke, Epilepsy, and Psychological Conditions
Multiple studies have reported associations between HRV (ECG analysis) and cognitive impairment in dementia, trauma, and COVID-19 (including EEG analysis).
3.2.1. Neurological Conditions
-
Dementia: The individual, social, and economic burden of dementia continues to grow. Alzheimer's disease (AD) is the most common type, followed by vascular dementia and dementia with Lewy bodies (DLB). Early detection, differential diagnosis, and the use of simple biomarkers are important for early prevention before overt symptoms appear. The Imbimbo research team (2022) studied 50 men and women (ages 51-77) with cardiovascular risk using 24-hour ECG, European Society of Cardiology cardiovascular risk assessment (ESC SCORE), and cognitive function (MoCA). This study showed that ULF HRV was positively correlated with MoCA and negatively correlated with ESC SCORE, meaning higher ULF HRV was associated with better cognitive function and lower ESC SCORE. This supports the idea that dysregulation of the autonomic nervous system plays an important role in cardiovascular risk and cognitive decline. A retrospective resting HRV study of patients with mild cognitive impairment (MCI) found that MCI patients who progressed to DLB (MCI-DLB) had lower HRV levels (SDNN, RMSSD, LF, HF) and lower visuospatial and frontal executive function on comprehensive neuropsychological testing compared to MCI patients who progressed to AD (MCI-AD). Another HRV study found that cognitive impairment (MMSE below 24) was more severe among participants with lower HRV (HF) in a sample of 311 elderly women. Thus, lower HRV was associated with cognitive decline. The Nicolini research team studied HRV in 253 participants including amnestic MCI (aMCI), non-amnestic MCI (naMCI), or cognitively normal controls. Traditionally, aMCI is associated with AD pathology and naMCI with other dementias such as vascular dementia. Among the three groups, the aMCI group showed blunted increase in normalized low frequency (nLF) with postural change (supine to standing), and nLF increase was associated with better episodic memory and less hippocampal/insular atrophy. This suggests overlapping autonomic regulation structures involved in memory processing. In contrast, naMCI participants showed HRV changes similar to controls, where LF increase was associated with greater cerebrovascular burden and lower executive function. These results suggest different autonomic mechanisms between aMCI and naMCI. Interestingly, HRV changes can vary by task type. For example, in a study of 80 elderly participants with MCI or healthy cognition, MCI participants showed smaller nLF increases and nHF decreases with postural change, indicating reduced physiological responsiveness when transitioning from supine to standing. The Arechavala team recorded 5-minute ECGs from cognitively healthy elderly participants at rest or during a computer-based task-switching paradigm. In the group with pathological amyloid/tau levels, HRV (RR and LF) decreased during the transition from rest to task, indicating excessive sympatho-vagal response to the task-switching paradigm. These studies suggest that individuals at early AD risk show diminished autonomic changes to physical postural changes but greater responses to mental tasks.
-
Mild traumatic brain injury (mTBI) or concussion: A study of 31 young athletes who experienced concussion or mTBI found that HRV (pNN50) decreased only during the acute phase (3 days post-injury) and recovered approximately 3 weeks later. Higher middle cerebral artery blood flow velocity in the acute phase was associated with higher HRV (pNN50) and better cognitive scores at 3 weeks and 3 months, suggesting that acute insular perfusion could be a potential predictor of future recovery.
-
Migraine: Migraine has been shown to be associated with autonomic dysfunction. A study of 18 episodic migraine patients and 18 controls found that migraine patients had lower SDNN and LF during attacks than controls. Lower HRV suggests parasympathetic dysfunction and was negatively correlated with pain intensity visual analog scale, meaning lower HRV was associated with greater pain intensity. The Matei research team analyzed 24-hour ECG HRV from 27 migraine patients and 10 healthy controls, observing consistent autonomic imbalance in migraine patients (especially those with nocturnal aura), including decreased SDNN, RMSSD, and HF, supporting parasympathetic dysfunction and sympathetic dominance. The Akter and Ferdousi team also studied 5-minute resting ECGs from 60 newly diagnosed migraine patients and 30 healthy controls, observing decreased SDNN and RMSSD and increased mean heart rate in the migraine group.
-
COVID-19 pandemic: COVID-19, a recent global health concern, also affected cognitive function. An online questionnaire and cognitive test completed by 421 participants found that memory deficits were associated with fatigue or complex symptoms. A retrospective study of 271 hospitalized patients showed that higher resting HRV (SDNN) predicted survival in COVID-19 patients over age 70. The Mol team confirmed that lower HRV predicted COVID-19 survival by age, supporting the protective role of vagal activity in COVID-19. Additionally, a study analyzing daily 5-7 minute ECG recordings over one week from 17 patients found that among 12 patients whose C-reactive protein (CRP) surged by more than 50%, 10 showed HRV (SDNN) decreases of 40% or more within 72 hours. This suggests that HRV decline predicts acute inflammation in COVID-19. Another study of 50 participants with COVID-19 history and 50 healthy controls showed decreased HRV in both time domain (SDNN, RMSSD) and frequency domain (LF, HF) after COVID-19, indicating HRV abnormalities. These studies suggest that HRV could be a useful tool for monitoring autonomic dysfunction in COVID-19 patients, though confirmation with larger sample sizes is needed.
-
Stroke: HRV can help predict stroke. A substudy of the Copenhagen Holter Study collected 48-hour ambulatory ECG and HRV from 678 healthy participants aged 55 to 75, finding that low nocturnal SDNN strongly predicted stroke occurrence even after adjusting for stroke risk factors. Another study examined baseline HRV in 5,308 patients with transient ischemic attack (TIA) and minor stroke, with 90-day follow-up of functional outcomes and stroke recurrence. Results suggest that higher SDNN predicts reduced neurological disability and fewer stroke events. A study of 884 stroke-free participants from the Cardiovascular Health Study (CHS) reported that HRV measures derived from 24-hour ECG -- CV% (coefficient of variation of each 5-minute NN interval) and SLOPE (power-law slope) -- significantly improved stroke prediction. Therefore, HRV is useful for stroke detection and prognosis.
-
Epilepsy: Epilepsy has been studied in relation to HRV for over 30 years. Patients' interictal HRV suggests autonomic balance shifts toward sympathetic dominance, tending toward additional sympathetic hyperactivity. A study of 11 epilepsy patients compared HRV from 5-minute ECG recordings 10-5 minutes before seizure onset versus 2 hours prior. Results showed increases in mean HR, LF/HF, and SD2/SD1 (Poincare plot nonlinear analysis ratios reflecting short- and long-term heart rate signal standard deviations) 5-10 minutes before seizure onset. These HRV features could potentially be used to define thresholds helpful for seizure prediction. A recent study of 41 patients with 238 temporal lobe epilepsy seizures also reported that HRV features including decreased RR and pNN50 helped identify pre-seizure states in 90% of patients and 41% of seizures.
3.2.2. Psychological Conditions
- Anxiety disorders: Anxiety disorders are associated with increased cardiovascular disease risk. A meta-analysis of 2,086 anxiety disorder patients and 2,294 controls without psychiatric diagnoses found that low HF and time-domain measures were associated with anxiety disorders. These results suggest that reduced vagal activity may be an underlying cause of increased cardiovascular risk in anxiety disorders.
- Stress conditions: A meta-analysis of 37 studies on HRV and stress suggested consistently low vagal activity associated with stress (decreased HF and increased LF).
- Schizophrenia: Schizophrenia, which particularly affects young people, has great epidemiological significance for healthcare systems in developed societies. The Schulz team studied cardiorespiratory network connectivity during 30-minute rest (NN intervals, heart rate, and respiratory frequency) in 23 schizophrenia patients, 20 first-degree relatives, and 23 healthy controls. Results suggested that in schizophrenia patients compared to controls, respiration had a weaker influence on heart rate, while heart rate had a stronger influence on respiration. Their first-degree relatives showed stronger heart rate influence. These results revealed a genetic component of cardiorespiratory coupling. The same team studied the central autonomic network (CAN) among central (frontal EEG power), vascular (systolic blood pressure amplitude), respiratory (frequency), and cardiac (heart rate) activities in 17 schizophrenia patients and 17 controls. Results suggested that schizophrenia patients showed stronger linear respiratory and cardiac influences on central activity and stronger linear central influences on vascular activity compared to controls. Therefore, HRV can be a potential objective measure of psychological distress including anxiety, stress, and schizophrenia.
HRV has been studied across diverse neurological conditions. HRV analysis can help predict symptoms or outcomes of cognitive decline, migraine, epilepsy, and stroke, and identify psychiatric pathologies such as anxiety, depression, and schizophrenia. These changes link pathology to symptoms, potentially allowing HRV to serve as a diagnostic and therapeutic adjunct in preclinical and clinical research.
In summary, higher HRV and its associated vagal function reflect better executive function, emotion regulation, and decision-making ability in healthy individuals. In pathological conditions, HRV was associated with autonomic dysfunction observed in neurological diseases. Efforts to improve our understanding of heart-brain interactions are needed.
FIGURE 3.
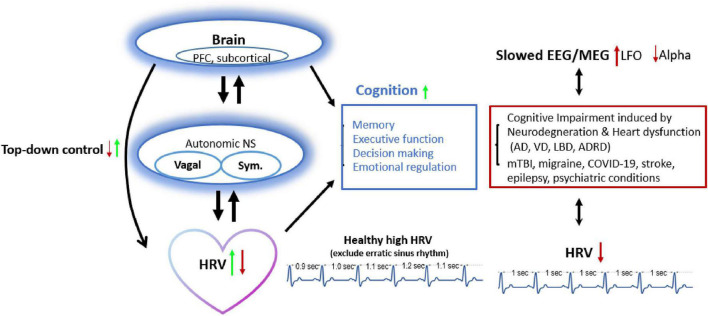 HRV and brain cognitive function have a bidirectional connection. Low HRV (due to reduced top-down inhibitory control) is linked to decreased executive function, decision-making, and emotion regulation, and is observed in pathological conditions (dementia, mild TBI, migraine, etc.). Approaches that increase HRV also improve brain activity (e.g., alpha frequency oscillations in the 8-12Hz range) and top-down control, and vice versa.
HRV and brain cognitive function have a bidirectional connection. Low HRV (due to reduced top-down inhibitory control) is linked to decreased executive function, decision-making, and emotion regulation, and is observed in pathological conditions (dementia, mild TBI, migraine, etc.). Approaches that increase HRV also improve brain activity (e.g., alpha frequency oscillations in the 8-12Hz range) and top-down control, and vice versa.
4. Updates and Limitations
There are several limitations and updates on this topic.
- Focus on linear HRV analysis: This review focused on linear analysis of HRV and did not include nonlinear HRV analysis.
- The role of heart rate fragmentation (HRF): While many studies focused on traditional HRV analysis representing autonomic regulation, recent studies have shown that more irregular sinus rhythms (erratic rhythm) can contribute to increased HRV in older adults beyond autonomic regulation. The underlying mechanisms of heart rate fragmentation are limited and may include cellular, intracellular, and extracellular mechanisms as well as potential desynchronization of sinoatrial node cells. Therefore, heart rate fragmentation adds complexity to interpreting HRV as neuro-autonomic regulation, consistent with a limited view of what HRV can tell us. Further research is needed.
- Diverse HRV measurement settings: We reviewed both short-term HRV measurement studies in laboratory settings (the majority) and long-term HRV measurement studies in real-world settings.
- Laboratory settings: Provide high-quality signals and individual responses to stimuli in controlled environments.
- Real-world settings: Have the advantage of processing stimuli in real life, but face challenges of signal quality degradation from physical activity and uncontrollable momentary conditions. Various approaches are being used to overcome these challenges, including additional noise-reduction algorithms, artificial intelligence, and appropriate baseline state usage. For example, carefully designed experiments that allow self-controlled data by collecting data from the same individual at different times or under different conditions are needed.
- Wearable sensors: Recent real-world HRV studies using wearable sensors have attracted attention, showing their utility as objective measures of stress or relaxation states and orthostatic challenges. HRV studies during virtual environment simulations have shown the ability to detect individuals vulnerable to stress.
- Caution in interpreting real-world HRV: HRV measured in real-world or free-living conditions must be interpreted carefully. Information at the time of measurement is often insufficient, and it is difficult to determine whether HRV analysis reflects characteristics of autonomic function or indirectly reflects characteristics of behavioral or psycho-physical activity. For example, low LF/HF during free-living conditions is associated with shorter life expectancy, but spending more time supine during the day may result in lower average LF/HF, which is unrelated to low sympathetic activity (low stress or better cardiac function).
5. Conclusion
The heart and brain have a critically important relationship in which they influence each other. Both are involved in appropriate responses to internal and external signals, supporting and regulating each other to help maintain our health and well-being. However, when this regulation is disrupted (e.g., decreased vagal function or increased HRF), it can be associated with cognitive impairment or other neurological conditions. Going forward, continued efforts to deepen our understanding of the fascinating interactions between heart and brain are essential.