This study is a systematic review and meta-analysis examining how continuous heart rate variability (HRV) monitoring has been used to understand stress and recovery patterns in doctors. The key finding is that several HRV parameters (RMSSD, SDNN, LF, LF/HF ratio) can detect statistically significant changes between stress and recovery periods, but the methodological heterogeneity and moderate study quality of current research make it difficult to draw definitive clinical conclusions. Future studies of higher quality and standardized measurement methods are needed, with particular emphasis on additional research involving UK medical workforce.
1. Introduction: Physician Burnout and the Need for HRV
Burnout has emerged as a serious problem among doctors in recent years. According to a 2023 UK General Medical Council (GMC) survey, 66% of trainees and 52% of trainers (senior doctors) reported moderate to high levels of burnout. The fact that 80% of emergency medicine and stroke medicine trainees experience severe burnout is particularly concerning.
"According to the 2023 UK GMC (General Medical Council) survey, among over 45,000 doctors, 66% of trainees and 52% of trainers (senior doctors) reported moderate to high levels of burnout."
Burnout is defined as a response to chronic workplace stress. Without adequate recovery, stress accumulates, becomes chronic, and can lead to burnout. While subjective methods currently exist for assessing recovery needs, the objective stress burden and recovery requirements of doctors remain poorly understood.
In this context, heart rate variability (HRV) has attracted attention as a promising objective measurement tool. HRV measures the subtle variations in intervals between heartbeats, reflecting autonomic nervous system activity. The sympathetic nervous system, associated with stress, decreases HRV, while the parasympathetic nervous system, associated with rest and recovery, increases HRV. Recently, wearable devices such as WHOOP!, Garmin, Fitbit, Oura, and Apple Watch have made HRV measurement accessible, extending its use to general wellness management. However, the simplified algorithms of these devices remain controversial.
HRV parameters reflect sympathetic and parasympathetic nervous system function and the overall balance of the autonomic nervous system, making them potentially useful biomarkers for measuring occupational stress and recovery in doctors through a non-invasive and cost-effective method. However, contextual or psychological measurements must accompany HRV measurement to distinguish between simple physiological stress responses and harmful stress responses.
This study aimed to evaluate research that combined continuous ambulatory HRV monitoring with contextual and subjective stress measurements to understand stress and recovery patterns in doctors.
2. Research Methods: Systematic Literature Review and Meta-Analysis
This study was conducted following rigorous systematic review and meta-analysis guidelines. The research protocol was pre-registered with PROSPERO (CRD42023413282) and followed the Cochrane Handbook and PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines.
2.1. Inclusion and Exclusion Criteria
- Inclusion criteria:
- Studies reporting at least one HRV parameter.
- A minimum of 10 participants.
- HRV measurement period of 24 hours or more.
- Studies including at least one contextual or psychological measurement alongside HRV.
- Studies involving doctors of various grades and specialties.
- Studies comparing stress and rest/recovery environments.
- Exclusion criteria:
- Studies with medical students as the primary research subjects.
- Studies conducting HRV monitoring in simulation or educational settings.
- Books, commentaries, editorials, guidelines, letters, news, opinions, reports, review articles.
- HRV monitoring of less than 24 hours.
| Category | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Study Design | All study types | Books, commentaries, editorials, guidelines, letters, news, opinions, reports, reviews |
| Participants | Minimum 10 participants, doctors of all grades and specialties | Medical students |
| Intervention/Exposure | Comparison of time spent in stress environments with rest, recovery, or less stressful states | No clearly defined stress environment, no clearly defined recovery or rest state |
| Comparison | All contextual or psychological measurements of stress and/or recovery | No comparison |
| Outcome | HRV monitoring of 24 hours or more | HRV monitoring of less than 24 hours |
2.2. Literature Search and Data Extraction
The literature search was conducted in June 2023 and repeated in July 2024. MEDLINE, Cochrane Library, Embase, and PsychINFO databases were used, along with grey literature from Google Scholar, MedArXiv, and PsyArXiv. The search scope covered 1982 to the present.
Retrieved titles and abstracts were imported into Covidence, deduplicated, and independently reviewed by two researchers (L.K., C.R.). Disagreements were resolved by a third researcher (J.C.). Full texts of finally selected papers were also reviewed in the same manner. Two papers published in languages other than English were translated before screening.
Data were extracted according to predefined criteria, including participant numbers, medical specialties, years of clinical experience, HRV measurement duration, HRV devices, defined stress and recovery periods, and HRV parameters.
2.3. Data Analysis
Initially, meta-analysis was expected to be difficult due to data heterogeneity, but after data extraction, it was determined that meta-analysis was feasible for five individual HRV parameters. Quantitative analysis used random effects analysis in RevMan (Web version 5.6.0, The Cochrane Collaboration). Results were presented as standardized mean differences (SMD) using the Hedges' adjusted g algorithm, with 95% confidence intervals (CI) reported. A P-value below 0.05 was considered statistically significant. Inter-study heterogeneity was assessed using I-squared scores.
Since all included studies met the Oxford Journal of Epidemiology's "case series" definition, study quality was assessed using the JBI (Joanna Briggs Institute) case series checklist and the Standards for Reporting Diagnostic Accuracy in HRV Research (STARDHRV).
3. Results: HRV Parameters and Stress-Recovery Relationships
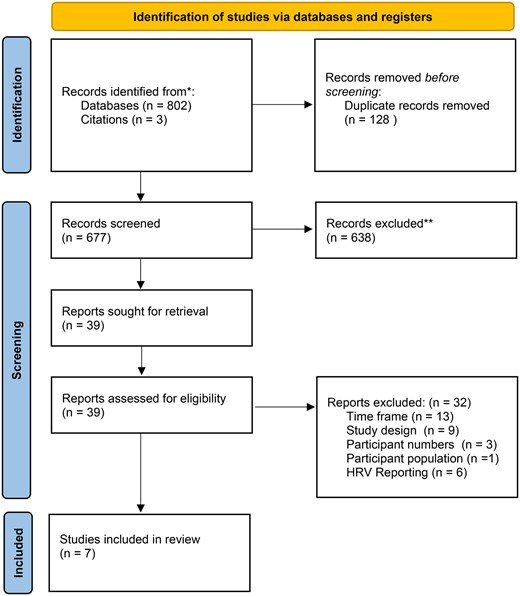
A total of 805 records were searched, and after deduplication and independent review, 39 full texts were reviewed. Ultimately, 7 studies met the inclusion criteria and were included in the systematic review.
3.1. Characteristics of Included Studies
The 7 selected studies were conducted in various countries including the Netherlands, Switzerland, Taiwan, Germany, Austria, Denmark, and Mexico, with a total of 176 participants. Participant numbers ranged from 12 to 54, and all studies used different HRV measurement devices.
- Stress periods: Varied, including surgical time, out-of-hospital emergencies, delivery room, and double shifts.
- Recovery periods: Variously defined as complete non-work rest, non-clinical administrative tasks, and off-duty time.
- Most stress and recovery periods were determined or assessed through self-report measurements.
- All studies measured HRV for 24 or 48 hours.

Figure 1. Flowchart following PRISMA methodology
3.2. Meta-Analysis Results: Significant Changes Between Stress and Recovery
Since no single common HRV parameter was reported across studies, subgroup analyses were performed by grouping studies based on HRV parameters reported for both stress and recovery periods.
-
RMSSD (Root Mean Square of Successive Differences):
- An HRV measure reflecting parasympathetic nervous system activity.
- Meta-analysis of 3 studies (43 participants) showed statistically significant differences in RMSSD between stress and recovery periods (Hedges g = -0.63, P = 0.005, 95% CI: -1.07, -0.19).
- Heterogeneity was low (I-squared = 0%).
-
SDNN (Standard Deviation of the NN (inter-beat) Intervals):
- Reflects both sympathetic and parasympathetic nervous system activity during short-term measurement, but better reflects sympathetic nervous system activity when measured for 24 hours or more.
- Meta-analysis of 4 studies (63 participants) showed statistically significant differences in SDNN between stress and recovery periods (Hedges g = -1.05, P = 0.001, 95% CI: -1.69, -0.41).
- Heterogeneity was moderate (I-squared = 64%).
-
HF (High Frequency):
- Reflects parasympathetic nervous system activity.
- Meta-analysis of 3 studies (43 participants) showed no statistically significant change in HF between stress and recovery periods (Hedges g = -0.24, P = 0.28, 95% CI: -0.68, -0.20).
- Heterogeneity was low (I-squared = 5%).
-
LF (Low Frequency):
- Reflects sympathetic nervous system activity.
- Meta-analysis of 3 studies (43 participants) showed statistically significant change in LF between stress and recovery groups (Hedges g = 0.54, P = 0.01, 95% CI: 0.11, 0.97).
- Heterogeneity was low (I-squared = 0%).
-
LF/HF Ratio:
- Reflects both sympathetic and parasympathetic nervous system function, with a high LF/HF ratio indicating sympathetic dominance.
- Meta-analysis of 2 studies (33 participants) showed statistically significant change in LF/HF ratio between stress and recovery groups (Hedges g = 0.69, P = 0.006, 95% CI: 0.19, 1.19).
- Heterogeneity was low (I-squared = 0%).

Figure 2. Random-effects meta-analysis assessing RMSSD, SDNN, HF, LF, and LF/HF HRV parameters as measures of stress and recovery
3.3. Study Quality Assessment
Study quality was assessed using the JBI checklist, and while all studies had high risk of bias, the overall risk of bias in studies included in the meta-analysis was low or uncertain. The highest risk of bias was found in the areas of "clear reporting of participant demographics" and "clear reporting of site demographic information."
HRV data measurement and reporting were assessed using the STARDHRV scale, with each study scoring between 9.5 and 14.5 out of 25. The highest completion rate was only 48%, and the lowest was just 24%. This suggests significant gaps in HRV reporting.
![Risk of bias [28] of studies included in the meta-analysis.](https://oup.silverchair-cdn.com/oup/backfile/Content_public/Journal/occmed/PAP/10.1093_occmed_kqaf101/1/m_kqaf101f3.jpeg?Expires=1764958175&Signature=wqYrP6I3zpOaONUuMySIUFQOPlPnlJ0sXY7AxrBKE9EDRYso~s0JVZ~XcXWgB4t8f56gdEBT1Jw9OoN0cUKrm~TYLI~BqkFeziqGt3FaoVDISMUQQ3nGnD43UZyAy7pPOUnhqfK3UtjlHqA76ANNlpzvH204kqYIFqI2o3ieTUj1xFy8eaqI0aJ6Yfhe0HG4Nu5ZIjAtpFV7tPe66ZmmkGIt83hCZFpbZOQaZOxEI0BGuD7tDqDvWCP0nRKnws7Xo5divTDh5FmjUK1jBNqdn6RB1p5dqJvldpKxO8VPT8L-bcE9QcYR0Hjn-SU0enUFPxApB4EwcQIp312Z3lfw__&Key-Pair-Id=APKAIE5G5CRDK6RD3PGA)
Figure 3. Risk of bias in studies included in the meta-analysis
4. Discussion: The Role of HRV Parameters and Future Research Directions
The key finding of this study is that among HRV parameters, SDNN, RMSSD, LF, and LF/HF ratio showed statistically significant changes between stress and recovery periods. The HF parameter did not show significant changes.
- SDNN: Reflects both sympathetic and parasympathetic nervous system function, showed a larger effect size, and may be more useful for detecting changes between stress and recovery states. It is known to be more accurate when measured for 24 hours or more.
- RMSSD: Better reflects parasympathetic nervous system function and may be useful for detecting acute stress. This is why it is popular in wearable technology.
- LF/HF ratio: Detects both sympathetic and parasympathetic nervous system function and showed a high effect size, but its role as an indicator of "sympatho-vagal balance" is controversial. It can be influenced by respiration and other factors.
- HF: Reflects only parasympathetic nervous activity, so it may be useful for detecting recovery states but is not suitable for detecting changes between stress and recovery, consistent with the findings of this study.
These results suggest that HRV parameters have potential for objectively monitoring occupational stress in doctors. However, the methodological heterogeneity and moderate study quality of current research are noted as major limitations.
In particular, because HRV analysis is influenced by various individual variables such as age, sex, health status, and physical activity level, it is crucial to adequately report participant demographic information. However, many studies lacked this information and did not follow HRV reporting standards (STARDHRV), making data interpretation difficult.
4.1. Strengths and Limitations
Strengths:
- Rigorously conducted following PRISMA guidelines, with the protocol pre-registered with PROSPERO.
- Includes 7 independent, international studies examining HRV during stress and recovery periods in doctors.
- Meta-analysis was possible for individual HRV parameters including RMSSD, SDNN, HF, LF, and LF/HF.
Limitations:
- The number of participants included in the meta-analysis was relatively small, with a maximum of 63 and minimum of 43.
- Heterogeneity was high for the SDNN parameter, and there were significant methodological differences between studies (e.g., different medical specialties, diverse stress/recovery environment definitions, different HRV measurement devices).
- Studies included in this review were conducted between 2009 and 2018, and wearable technology has advanced significantly since then. Current wrist-worn or ring-type wearable devices may face additional challenges for HRV measurement due to age-related vascular stiffness, skin color, and infection control regulations for doctors (prohibiting watches or rings). Therefore, ECG-based chest-worn devices may be more suitable for high-quality HRV measurement.
- Chronic stress and burnout accumulate over long periods, but the measurement periods in the included studies were relatively short at 24 to 48 hours, limiting understanding of long-term occupational stress patterns.
- Continuous HRV measurement and self-reporting can trigger measurement reactivity, potentially leading to behavioral changes.
4.2. Recommendations for Future Research
Future research should address the following improvements:
- Higher quality studies are needed, particularly research involving UK medical workforce.
- Robust baseline methodologies should be established, following European Task Force HRV research guidelines and STARDHRV reporting standards.
- Participant demographic reporting and within-person design should be strengthened to better understand how HRV can serve as a personalized health indicator.
- Methods should be explored to prevent participant behavioral changes by not providing immediate biofeedback and to reduce measurement reactivity by repeating self-report measurements throughout the study period.
- Latest HRV technology should be utilized to collect data over longer measurement periods to better understand the long-term patterns contributing to occupational stress and burnout.
Conclusion: The Potential of HRV for Physician Burnout Management
This systematic review and meta-analysis demonstrated that HRV parameters such as RMSSD, SDNN, LF, and LF/HF ratio can detect statistically significant changes between stress and recovery states in doctors' typical clinical environments. This suggests that HRV monitoring has the potential to become an important tool for preventing and managing burnout by objectively tracking occupational stress and recovery patterns in doctors.
However, current studies have limitations including relatively small sample sizes, methodological heterogeneity, and moderate study quality. Therefore, it is currently difficult to draw meaningful clinical conclusions. The minimum clinically important difference in HRV between stress and recovery that would positively reduce burnout risk remains unknown.
In conclusion, future high-quality studies with robust measurement techniques and comprehensive HRV parameter reporting that comply with European Task Force and STARDHRV guidelines are urgently needed. Such studies will increase the clinical applicability of providing occupational health professionals with objective tools for detecting and monitoring stress-related responses in doctors, ultimately contributing to reducing physician burnout.